
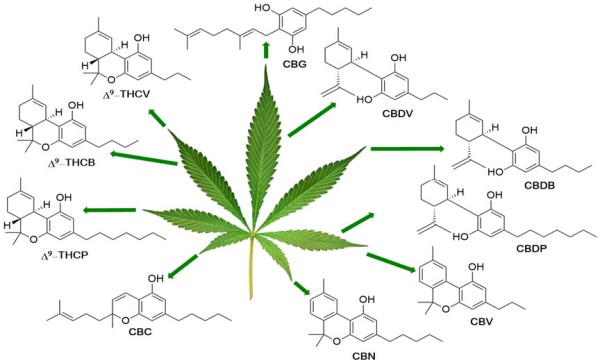
Δ-9-tetrahydrocannabinol (THC) and cannabidiol (CBD), the major active compounds of the plant Cannabis sativa (cannabis), are substances with a significant therapeutic potential and increasing clinical applications. The effects of THC and CBD (range, intensity, location and length) depend mainly on their pharmacology: presentation, administration route and dosage. In this context cannabinoid pharmacology offers interesting options for the development of precise and specific therapeutic strategies adaptable to many clinics.
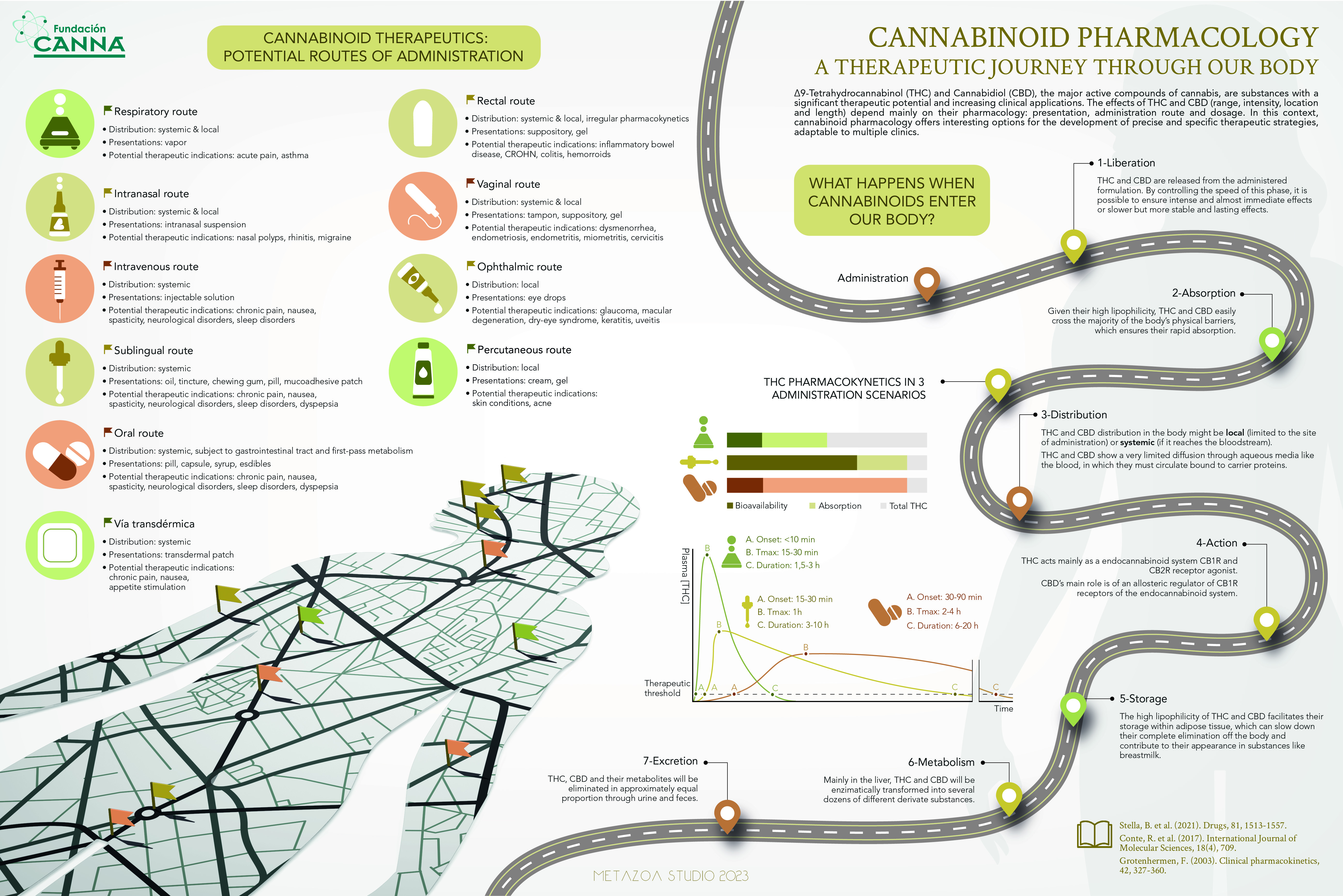
What happens when cannabinoids enter the body?
 Following administration, THC and CBD are released from the administered formulation. By controlling the speed of this phase, it is possible to ensure intense and almost immediate effects or slower but more stable and lasting effects.
Following administration, THC and CBD are released from the administered formulation. By controlling the speed of this phase, it is possible to ensure intense and almost immediate effects or slower but more stable and lasting effects.- After release, given their high lipophilicity (ability to dissolve more easily in lipids [a class of oily organic compounds] than in water), THC and CBD easily cross the majority of the body’s physical barriers, which ensures their rapid absorption.
- Following absorption, THC and CBD distribution in the body may be local (limited to the site of administration) or systemic (if it reaches the bloodstream). THC and CBD show a very limited diffusion through the aqueous (water-like) media like the blood, in which they must circulate bound to carrier proteins.
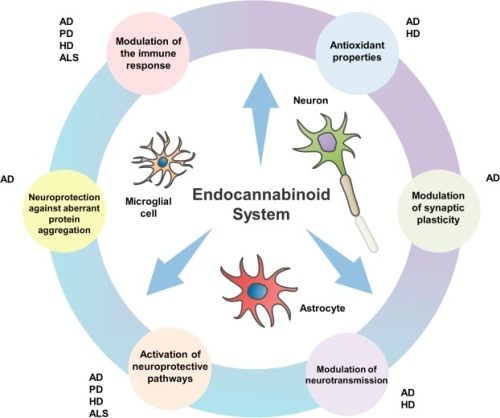
- After distribution, THC acts mainly as an endocannabinoid system CB1 receptor and CB2 receptor agonist (substance which initiates a physiological response when combined with a receptor). CBD’s main role is of an allosteric regulator (increasing or decreasing affinity of the receptor for other molecules) of CB1 receptors of the endocannabinoid system.
- Following the action of these cannabinoids, the high lipophilicity of THC and CBD facilitates their storage within adipose tissue (connective tissue consisting largely of fat cells), which can slow down their complete elimination from the body and contribute to their appearance in substances like breast milk.
- Metabolism occurs mainly in the liver, where THC and CBD are enzymatically (involving enzymes [chemical substances produced by living cells that cause particular chemical reactions to happen while remaining unchanged themselves) transformed into several dozens of different derivative substances.
- Excretion of THC, CBD and their metabolites will be in approximately equal proportion through urine and faeces and may take up to five days for 80-90% of the total dose to be excreted.
Cannabinoid Therapeutics: Potential Routes of Administration
The general principle should be to start low and go slow. Cannabis-naïve patients may
only need between 0.1–0.5 of the starting dose of a regular cannabis user to note effects.
|
|
|
|
|
|
|
|
|
|
|
|
|
Medicinal cannabis consumed as oils or liquid capsules are more slowly absorbed. Effects are generally delayed for 30-90 minutes. Bioavailability of oral cannabinoids is low (10-20%) because of intestinal and first pass liver metabolism. Peak effects can occur two to four hours after consumption. Allow at least three hours between administration of single oral doses. Effects can last eight to as long as 24 hours. |
|
|
Given the slower onset and longer duration, taking medicinal cannabis orally would be more useful for conditions or symptoms where control over longer periods of time is sought – similar to use of slow release medications. Sprays appear to have a similar mode of action, as some of the product is swallowed. Effects typically start at 90 minutes after administration and last about the same time as orally administered cannabinoids. Titration of dose may be easier with oromucosal spray than oral formulations. |
|
|
|
|
|
THC is not generally well absorbed through the skin. CBD and cannabinol (CBN) are 10 times more permeable than THC and are more likely to be used in topical preparations. The time of onset and duration of action are unknown. |
|
|
|
|
|
|
|
|
In Australia, the two pictured vaporisers are suggested for use by the Therapeutic Goods Administration (TGA), which is the largely self-funded authority that operates on a cost recovery basis (part of the Australian Government Department of Health), charging fees for services (such as evaluating a new product) and imposing annual charges on industry. The following is adapted from the TGA’s ‘Guidance for the use of medicinal cannabis in Australia’: |
|
|
|
|
|
|
|
|
|
|
|
|
 |









Adapted from Cannabinoid Pharmacology. A therapeutic journey through our body by Fundación CANNA

{kind=link}