


Driving Under the Influence of Cannabis: Impact of Combining
Toxicology Testing with Field Sobriety Tests
United States (USA), July 2023
The relationship between cannabis use and driving impairment is complex because of the unique pharmacokinetic (how the body interacts with administered substances for duration of exposure) and pharmacodynamic (biochemical and physiologic) properties of cannabis’ ∆9-tetrahydrocannabinol (∆9-THC). Impairment is difficult to define because there is no universally agreed-upon task that can be used to define driving impairment. The relationship between blood ∆9-THC concentrations and crash risk is not established, but there is a clear understanding that ∆9-THC impairs driving performance in many, but not necessarily all, individuals. The question that remains is how to best identify drivers who are impaired by cannabis.
In the largest trial to date involving experienced users smoking cannabis, there was
no correlation between ∆9-THC in blood, oral fluid, or breath and driving performance.
The complete lack of a relationship between the concentration of the centrally active component of
cannabis in blood, oral fluid and breath is strong evidence against use of ‘per se’ laws for cannabis.
Driving under the influence of cannabis, alcohol, and illicit drugs
among adults in the United States from 2016 to 2020
USA, May 2023
Greater than one in ten USA adults reported Driving Under the Influence (DUI) of any substance annually from 2016 to 2020. DUIA (alcohol) was most prevalent among all USA adults; however, this behaviour is decreasing. No change in DUIC was found among the USA adult population, but a decrease was found among those with past-year cannabis use which coincided with a 29.1% increase in past-year cannabis use. There were no significant changes in overall DUID (drugs); however, females aged 26-34 and 65 or older with past-year use displayed increasing trends. DUI of any substance decreased among the USA adult population.

Contemporary drug use and driving patterns: A qualitative approach to understanding drug-driving perceptions from the context of user patterns
Australia, November 2022
This study aimed to identify the typologies of substance users and examine how they differed in drug-driving tendencies. Thematic analyses identified three unique user types: a) sporadic recreational users, who used a variety of ‘drugs’ and drove, depending on situational variables; b) frequent recreational users, who favoured cannabis and methamphetamine, and did not typically regulate their driving; and c) frequent medicinal users, who used cannabis for a medical condition and were more responsible in regulating both their use and driving. While frequent recreational users may ‘drug drive’ more often, sporadic users (who are proportionally larger in size) may be more at risk due to a low tolerance and an increased likelihood of poly-substance use. The findings of this study may inform the development of tailored police interventions but also inform current policy discussions.
Consistent with an improvement in traffic safety, the legalisation of medical cannabis leads to a decrease in auto insurance premiums on average of US$22 (>AU$33) per policy, per year. The effect is stronger in areas directly exposed to a dispensary, suggesting increased access to cannabis drives the results. In addition, relatively large declines in premiums seen in areas with relatively high drunk driving rates prior to medical cannabis legalisation. This latter result is consistent with substitutability across substances that is argued in the literature.

Indeterminacy of cannabis impairment and
∆9-tetrahydrocannabinol levels in blood and breath
USA, May 2022
Previous investigators found no clear relationship between specific blood concentrations of ∆9-THC and impairment, and thus no scientific justification for use of legal ‘per se’ ∆9-THC blood concentration limits. Analysing blood from 30 subjects showed ∆9-THC concentrations that exceeded 5 ng/mL in 16 of the 30 subjects following a 12-hour period of abstinence in the absence of any impairment. In blood and exhaled breath samples collected from a group of 34 subjects at baseline prior to smoking, increasing breath ∆9-THC levels were correlated with increasing blood levels in the absence of impairment, suggesting that single measurements of ∆9-THC in breath, as in blood, are not related to impairment.

Driving Performance and Cannabis Users’ Perception of Safety
USA, January 2022
In a randomised clinical trial, 191 regular cannabis users smoked ad libitum placebo, 5.9% or 13.4% ∆9-THC cigarettes. Simulator driving worsened in the ∆9-THC group, but this was unrelated to ∆9-THC content, use history, or blood ∆9-THC concentration. Perception of driving impairment decreased at 1 hour 30 minutes, despite no objective improvement in driving; on average, performance was indistinguishable from placebo group at 4 hours 30 minutes. When experienced cannabis users control their own intake, one cannot infer impairment based on the product ∆9-THC content or blood concentrations.
There was no correlation between blood ∆9-THC concentrations collected 15 minutes after smoking and
simulator performance at 30 minutes or any other time point … under highly controlled conditions.

In the real world, the time from consumption to a law enforcement stop and
subsequent blood collections is highly variable, and the current results reinforce
that ‘per se’ laws based on blood ∆9-THC concentrations are not supported.
State ‘Marijuana’* Laws and Traffic Fatalities
USA, December 2021
Researchers examined the relationship between traffic fatalities and state cannabis laws using data from 1985 to 2019 and found lower state traffic fatalities following the implementation of medical cannabis laws. This is true whether a simple medical cannabis law indicator or a continuous indicator of the permissiveness of state medical cannabis laws is employed. Controlling for prior medical cannabis laws, there was no evidence of a statistically significant association found between recreational cannabis laws and traffic fatalities as of 2019. Liberalisation has been associated with lower traffic fatalities, not higher.

The risk of being culpable for or involved in a road crash after
using cannabis: A systematic review and meta-analyses
Australia, December 2021
Researchers undertook a systematic search of electronic databases and identified 13 culpability studies and four case–control studies from which cannabis-crash odds ratios could be extracted. It was evident that the risks from driving after using cannabis are much lower than from other behaviours such as drink-driving, speeding or using mobile phones while driving. With medical and recreational use of cannabis becoming more prevalent, removal of cannabis-presence driving offences should be considered (while impairment-based offences should remain).

Are blood and oral fluid Δ9-THC and metabolite concentrations
related to impairment? A meta-regression analysis
Australia, November 2021
Researchers performed a meta-analysis to characterise the relationships between ∆9-THC-related biomarkers, subjective ‘intoxication’ and impairment of driving and driving-related cognitive skills in regular and occasional cannabis users. Blood ∆9-THC, 11−OH-THC and 11−COOH-THC concentrations, oral fluid ∆9-THC concentrations and subjective ratings of ‘intoxication’ are relatively poor indicators of cannabis-induced impairment. Use of ‘per se’ limits as a means of identifying cannabis-impaired drivers should be reconsidered. It seems there is a significant risk of unimpaired individuals being mistakenly identified as ‘cannabis-impaired’ (and vice-versa) under this approach.

Cannabis and Driving
USA, September 2021
Current evidence suggests that efforts to establish ‘per se’ limits for cannabis-impaired drivers based on blood ∆9-THC values are still premature at this time. Considerably more evidence is needed before there can be an equivalent to a blood alcohol concentration, a ‘BAC for THC’. The particular pharmacokinetics of cannabis and its variable impairing effects on driving ability currently seem to argue that defining a standardised ‘per se’ limit for ∆9-THC will be a very difficult goal to achieve.

The failings of ‘per se’ limits to detect cannabis-induced driving
impairment: Results from a simulated driving study
Australia, February 2021
Due to erratic and route-dependent differences in ∆9-THC pharmacokinetics as well as significant inter- and intra-individual variability, blood and oral fluid ∆9-THC concentrations, unlike BAC for alcohol, provide little information as to the amount of cannabis consumed or the extent to which an individual may be ‘intoxicated’. Collectively, these results suggest the ‘per se’ limits examined here do not reliably represent thresholds for impaired driving.

Cannabis and driving ability
USA, 2021
This review examines experimental research on the acute effects of ∆9-THC on driving-related neurobehavioural skills and driving performance based on simulator and road course studies. The evidence indicates that certain driving abilities are significantly, albeit modestly, impaired in individuals experiencing the acute effects of ∆9-THC. Treatment effects are moderated by dose, delivery method, recency of use and tolerance development.
Current research indicates biological ∆9-THC concentrations are not strongly
correlated with impairment, so ‘per se’ laws that criminalise driving above
specific thresholds do not appear to be justified as stand-alone policy.

New DUI and DUID research studies should consider key issues in the study design, including the time elapsed since the substance use; the method of administration; dosage; and most importantly, how test results relate to impaired driving, including the best methods to identify impaired drivers. Drugs affect people differently depending on many variables. A ‘per se’ limit for drugs, other than ethanol, should not be enacted at this time as current scientific research does not support it.

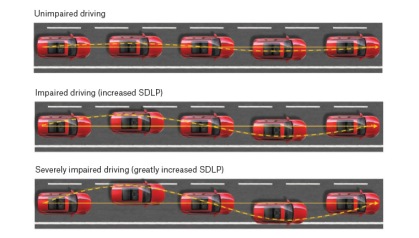
Effect of Cannabidiol and Δ9-Tetrahydrocannabinol on Driving Performance
Australia/The Netherlands, December 2020
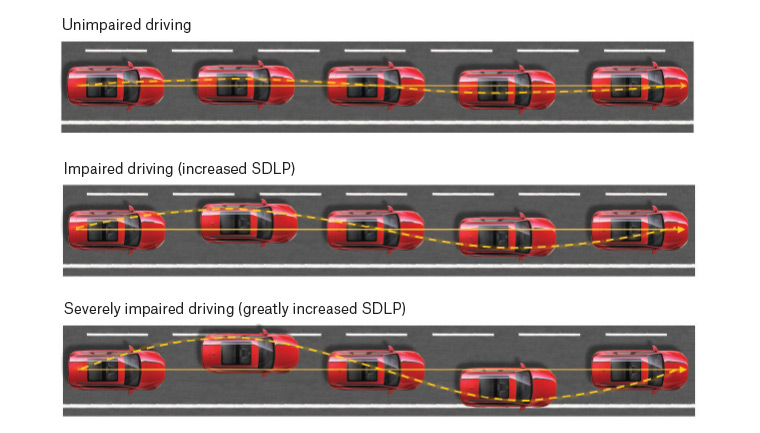
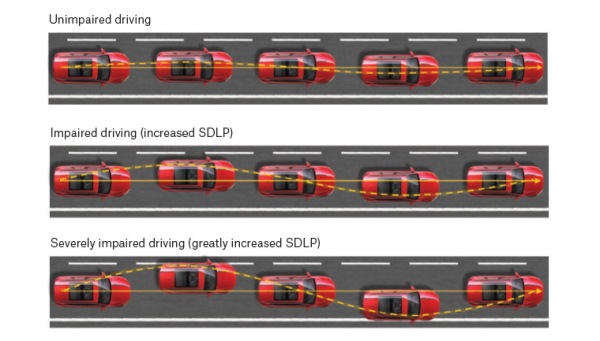
In a crossover clinical trial that assessed driving performance during on-road driving tests, the standard deviation of the lateral position (SDLP) following vaporised ∆9-THC-dominant and ∆9-THC/CBD-equivalent cannabis compared with placebo was significantly greater at 40-100 minutes but not 240-300 minutes after vaporisation; there were no significant differences between CBD-dominant cannabis and placebo.

An examination of relationships between cannabis legalisation
and fatal motor vehicle and pedestrian-involved crashes
USA, August 2020
There has been limited research on how cannabis affects pedestrians involved in traffic crashes. This study examined the association between cannabis legalisation (medical, recreational use and recreational sales) and fatal motor vehicle crash rates (both pedestrian-involved and total fatal crashes). No significant differences in pedestrian-involved fatal motor vehicle crashes between legalised cannabis states and control states following medical or recreational cannabis legalisation were found. Washington and Oregon saw immediate decreases in all fatal crashes following medical cannabis legalisation. Overall findings do not suggest an elevated risk of total or pedestrian-involved fatal motor vehicle crashes.

Residual blood ∆9-THC levels in frequent cannabis users after
over four hours of abstinence: A systematic review
Canada, June 2020
Epidemiological evidence supporting a specific ‘per se’ limit for ∆9-THC is scant. Blood ∆9-THC >2ng/mL and possibly even ∆9-THC >5ng/mL does not necessarily represent recent use of cannabis in frequent cannabis users. People who use cannabis regularly develop partial tolerance to some of its impairing effects. Regular cannabis users may also have persistent elevation of ∆9-THC even after a period of abstinence. Some stakeholders worry that current ‘per se’ limits may criminalise unimpaired drivers simply because they use cannabis.
Acute and residual effects of smoked cannabis: Impact on driving speed
and lateral control, heart rate, and self-reported drug effects
Canada, December 2019
In a double-blind, placebo-controlled, parallel-group, randomised clinical trial, 30 high ∆9-THC, 31 low ∆9-THC and 30 placebo subjects were studied. Mean speed (but not lateral control) significantly differed between groups 30 minutes after smoking cannabis with low and high ∆9-THC groups decreasing speed, compared to placebo. Heart rate, visual analogue scale (VAS) drug effect and drug high increased significantly immediately after smoking cannabis and declined steadily thereafter. There was little evidence of residual effects in any of the measures.

Strengths and limitations of two cannabis-impaired driving
detection methods: a review of the literature
USA, September 2019
The relationship between crash risk and amount of cannabis consumed or blood concentration of ∆9-THC is weak. Blood concentration of ∆9-THC is a poor index of driving-related risk or impairment. Although standard field sobriety tests have advantages over ‘per se’ tests for cannabis-impaired driving, limitations of both leave cannabis users and law enforcement officials little guidance in assessing an individual’s driving fitness after recent cannabis use.

Cannabis use as a risk factor for causing motor
vehicle crashes: a prospective study
Canada, July 2019
In British Columbia, non-fatally injured motor vehicle drivers’ toxicology results (3,005) and police reports (2,318) showed alcohol was detected in 14.4%, Δ9-THC in 8.3%, other drugs in 8.9% and sedating medications in 19.8%. There was no evidence of increased crash risk in drivers with Δ9-THC <5ng/ml and a statistically non-significant increased risk of crash responsibility in drivers with Δ9-THC ≥5ng/ml.

Cannabidiol (CBD) content in vaporised cannabis does not
prevent ∆9-THC-induced impairment of driving and cognition
Australia, May 2019
In a randomised, double-blind, within-subjects crossover design study, healthy volunteers with a history of light cannabis use attended three simulated driving and cognitive performance test sessions. They were assessed at 20–60 minutes and 200–240 minutes following vaporisation of 125mg ∆9-THC-dominant, (11% ∆9-THC:<1% CBD), ∆9-THC/CBD equivalent (11% ∆9-THC:11% CBD) or placebo (<1% ∆9-THC/CBD) cannabis. Cannabis containing equivalent concentrations of CBD and ∆9-THC appears no less impairing than ∆9-THC-dominant cannabis. Both active cannabis types increased intra-lane weaving during a car-following task but had little effect on other driving performance measures.

Levels of impairment identified in laboratory settings may not have a significant impact in real world settings, where many variables affect likelihood of a crash occurring. Research has been unable to consistently correlate levels of cannabis consumption, or ∆9-THC in a person’s body, and levels of impairment. Some researchers, and the National Highway Traffic Safety Administration, observed that using a measure of ∆9-THC as evidence of a driver’s impairment is not supported by scientific evidence to date.
Effect of Smoked Cannabis on Vigilance and Accident Risk Using
Simulated Driving in Occasional and Chronic Users and
Pharmacokinetic-Pharmacodynamic Relationship
France, March 2019
The pharmacokinetic-pharmacodynamic relationship between whole blood ∆9-THC and driving risk is poorly understood. In a randomised, double-blind, crossover trial, 15 chronic consumers and 15 occasional consumers, aged 18-34 were studied. Results showed that inhalation from cannabis joints leads to a rapid increase in blood ∆9-THC with a delayed decrease in vigilance and driving performance, more pronounced and lasting longer in occasional consumers than in chronic consumers.

On the impact of cannabis consumption on traffic safety:
a driving simulator study with habitual cannabis consumers
Germany, January 2019
A driving simulator study with habitually cannabis consuming test persons was conducted to contribute to the ongoing discussion about threshold limits of Δ9-THC. Consistent with previous studies, a direct correlation between individual fitness to drive and ∆9-THC concentrations was not found. Therefore, determining a threshold limit for legal purposes based on these values alone seems to be arbitrary.
‘Marijuana’* medicalisation and motor vehicle fatalities:
a synthetic control group approach
USA, December 2018
A quasi-experimental evaluation of California’s 1996 medical cannabis law, known as Proposition 215, was performed on statewide motor vehicle fatalities between 1996 and 2015. California’s 1996 medical cannabis law appears to have produced a large, sustained decrease in statewide motor vehicle fatalities amounting to an annual reduction between 588 and 900 vehicle fatalities

Legalising medical cannabis in California led to a sustained reduction in statewide motor vehicle fatalities.

Cannabis use and driving-related performance in young recreational
users: a within-subject randomised clinical trial
Canada, October 2018
Randomised, within-subjects trial with assessors being blinded to time since cannabis use, and participants blinded to randomisation sequence. Among young recreational cannabis users, a 100-mg dose of cannabis by inhalation had no effect on simple driving-related tasks, but there was significant impairment on complex tasks, especially when these were novel. These effects, along with lower self-perceived driving ability and safety, lasted up to five hours after use.

Driving While Stoned: Issues and Policy Options
USA, July 2018
An analysis and research white paper concluded that even if cannabis impairment is present, it creates (unless combined with alcohol or other drugs) only a fraction of the risks associated with driving at the legal 0.08 BAC threshold, let alone the much higher risks associated with higher levels of alcohol. The maximum risk for cannabis ‘intoxication’ alone, unmixed with alcohol or other drugs, appears to be more comparable to risks such as talking on a hands-free phone (legal in all USA states) than to driving with a BAC above 0.08, let alone rapidly-rising risks at higher BACs.

*Cannabis sativa is the correct botanical term, ‘marijuana’ is an American colloquialism, at best













 Malmo-Levine continued,
Malmo-Levine continued, 
























 The
The 
 more roles for their already over-inflated, taxpayer-funded bureaucracy. Politics should not, again, enter the picture. Canada doesn’t need parliamentarians constantly creating new laws and regulations and then empowering expensive bureaucracies to enforce them.
more roles for their already over-inflated, taxpayer-funded bureaucracy. Politics should not, again, enter the picture. Canada doesn’t need parliamentarians constantly creating new laws and regulations and then empowering expensive bureaucracies to enforce them. In 2000, the Supreme Court of Canada ruled Canadians had the constitutional right to use cannabis as medicine. This change in the law gave medical patients the right to use bud and plant material only. In 2012 in Victoria, British Columbia (BC), a medical cannabis bakery was busted by police. The baker, Owen Smith, was arrested and charged with trafficking. Thankfully, he fought the charges. The 2015 court decision from
In 2000, the Supreme Court of Canada ruled Canadians had the constitutional right to use cannabis as medicine. This change in the law gave medical patients the right to use bud and plant material only. In 2012 in Victoria, British Columbia (BC), a medical cannabis bakery was busted by police. The baker, Owen Smith, was arrested and charged with trafficking. Thankfully, he fought the charges. The 2015 court decision from 
 This restriction infringed the right to liberty and the right to security in an arbitrary manner. Since arbitrariness goes against the principles of fundamental justice that underpin s. 7 of the Charter, this was deemed unacceptable. Although the intended goal of the prohibition was mitigation of health and safety concerns, the SCC felt it had a different effect, forcing people who had a legally recognised need, to accept the risk of harm to their health that comes with smoking instead of administering it through a different method in a non-dried form.
This restriction infringed the right to liberty and the right to security in an arbitrary manner. Since arbitrariness goes against the principles of fundamental justice that underpin s. 7 of the Charter, this was deemed unacceptable. Although the intended goal of the prohibition was mitigation of health and safety concerns, the SCC felt it had a different effect, forcing people who had a legally recognised need, to accept the risk of harm to their health that comes with smoking instead of administering it through a different method in a non-dried form.





 An Australian
An Australian 
 In 2021, however, fewer than 3% of California’s more than 78,000 sworn police officers were trained as Drug Recognition Evaluators (DREs). California plans to train more and the CHP’s Impaired Driving Task Force called for increasing the number of DRE-trained officers to 7% (over five years). The Task Force also called to extend the required standardised field sobriety training from 8 to 24 hours, helping to improve detection of impaired drivers in roadside tests and help create safer roads. These measures could serve as an example of how fair and just drug driving laws can be adopted to move past methods proven outdated and inconsistent. California (population: 39 million) serves as a relatable example to Australia (25 million people).
In 2021, however, fewer than 3% of California’s more than 78,000 sworn police officers were trained as Drug Recognition Evaluators (DREs). California plans to train more and the CHP’s Impaired Driving Task Force called for increasing the number of DRE-trained officers to 7% (over five years). The Task Force also called to extend the required standardised field sobriety training from 8 to 24 hours, helping to improve detection of impaired drivers in roadside tests and help create safer roads. These measures could serve as an example of how fair and just drug driving laws can be adopted to move past methods proven outdated and inconsistent. California (population: 39 million) serves as a relatable example to Australia (25 million people). How does roadside detection of cannabis-impaired drivers unfold in reality in the US?
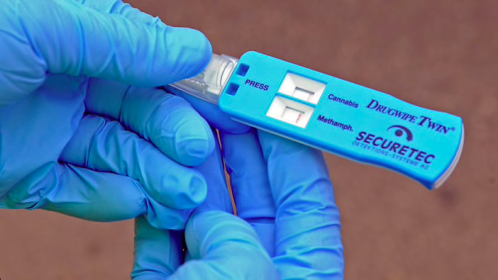
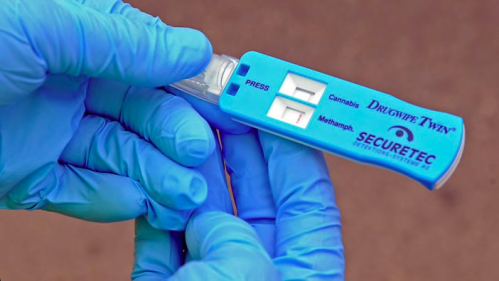
How does roadside detection of cannabis-impaired drivers unfold in reality in the US?




 A recent sign that there’s a fundamental change going on in the detection of cannabis impairment came in the form of a
A recent sign that there’s a fundamental change going on in the detection of cannabis impairment came in the form of a 



 A statement from the school hailed hemp fibre as a reinforcement and alternative to synthetic fibres such as glass; “The fibres are a renewable source, making natural fibre composites particularly attractive from an environmental standpoint”. Materials developed from hemp fibres had a higher strength-to-weight ratio than steel. For the past 20-25 years, Australian researchers have revived breeding stock and farming of hemp. Value addition through research has led to substantial growth in the Australian hemp export industry. In 2016, in the
A statement from the school hailed hemp fibre as a reinforcement and alternative to synthetic fibres such as glass; “The fibres are a renewable source, making natural fibre composites particularly attractive from an environmental standpoint”. Materials developed from hemp fibres had a higher strength-to-weight ratio than steel. For the past 20-25 years, Australian researchers have revived breeding stock and farming of hemp. Value addition through research has led to substantial growth in the Australian hemp export industry. In 2016, in the 

 After being wrapped in red-tape for nearly a century, hemp is still considered taboo. Unfortunately, due to its similarity to cannabis, people are still uncertain and wary. The
After being wrapped in red-tape for nearly a century, hemp is still considered taboo. Unfortunately, due to its similarity to cannabis, people are still uncertain and wary. The 
 The Trials incorporate seven sites (see map), with sowing commencing in October 2021 in the five central and southern regions. The two northern sites will commence sowing later in 2022 due to latitude, day length and climatic differences.
The Trials incorporate seven sites (see map), with sowing commencing in October 2021 in the five central and southern regions. The two northern sites will commence sowing later in 2022 due to latitude, day length and climatic differences. 






